|
We've spent the last few Muscle Mondays focusing on the upper body, particularly about posture and how it affects our muscles and joints. Let's take a moment and look at one of the integral team members of our "core" and a common culprit for low back-related issues. Allow me to introduce to you, the Psoas Major (silent "P"). 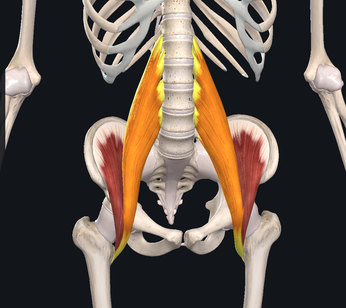 While there are many unique features about this muscle, perhaps the most significant is the number of joints that it crosses. This muscle originates at the transverse processes of T12-L4, crossing 5 spinal segments before going distally and inserting into the lesser trochanter of the femur. Because it crosses so many joints, it is responsible for 3 main movements including: Lumbar flexion, ipsilateral side-bend and hip flexion. Because of its attachment on the inside of the thigh, it also will slightly externally rotate the femur as well. Trunk/Lumbar flexion Trunk/Lumbar Sidebend Hip Flexion The primary job of the Psoas is to flex the hip. It joins together with the iliacus muscle to form the iliopsoas tendon. 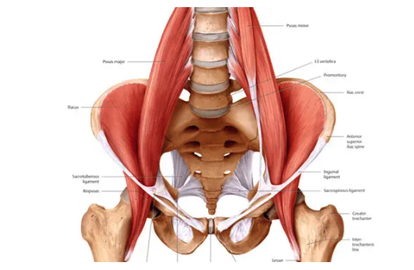 One of the main issues that people commonly face, particularly those who have a more sedentary lifestyle or job that requires several hours of sitting, is that the muscle will gradually adapt and shorten over time. Why this is an issue, is that this can result on increased stress on the lower back when you try and stand up tall/straight due to the tightness of the muscle which naturally would pull you into more trunk and hip flexion. In order to compensate, you would extend (or arch) your back more to allow you to get into the full upright position. Other common issues related to the psoas major are hip flexor tendinitis and/or "snapping hip syndrome" (the two are NOT synonymous). Hip flexor tendinitis describes an acute inflammation of the iliopsoas tendon and commonly painful with active contraction of the hip flexors. On the other hand, snapping hip syndrome is a condition in which a person may experience or hear a popping/snapping sensation in the front of their hip when they flex their hip, but may or may not be painful when the sensation occurs. Snapping hip syndrome typically indicates that there is friction on the tendon (which causes the "snap"). It could potentially lead to tendinitis and scar tissue formation of the iliopsoas tendon. Both of these conditions are commonly found in dancers, bikers, soccer players and runners. One quick and simple way to check to see if you have tight hip flexors is to perform a Thomas Test. While this is most commonly performed by a healthcare professional in the clinic, it is simple to do and can offer helpful insight to help you fine tune your body. To perform, you lay down on a bed while hugging one knee towards your chest. The other leg (the one you are testing) would drop down towards to floor. If you feel your back start to arch up, or if your femur (thigh) does not reach parallel to the floor, it would suggest that you have tightness/stiffness of your hip flexors. Do not, however, perform this if you are unsteady (in other words, don't fall off the bed), or if you already have pain in the area. Please make sure to seek advice from a medical professional for more detailed assessment. 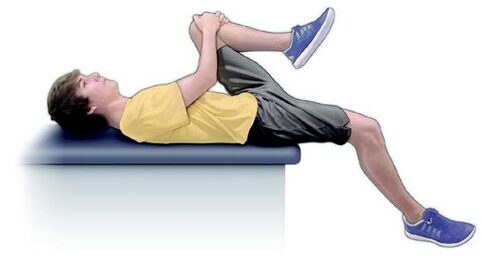 One very simple and easy place to start would be to start a simple stretching and strengthening regimen. Follow along in the video below to learn one of my all-time favorite stretches that I personally do on a daily basis. Of course, this is all about balance. Not only is stretching largely advisable to help maintain good habits, but it is also important to strengthen the appropriate muscles as well. In this particular case, it is important to focus on the glutes (Max, Med). Make sure that if you sit for work or school, that you get up and stretch a couple of minutes or walk around every hour. As always, check in with your friendly neighborhood physical therapist for specific guidance and tips to help you keep your body in prime working condition.
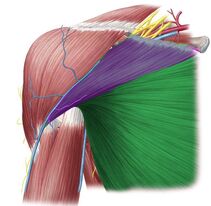
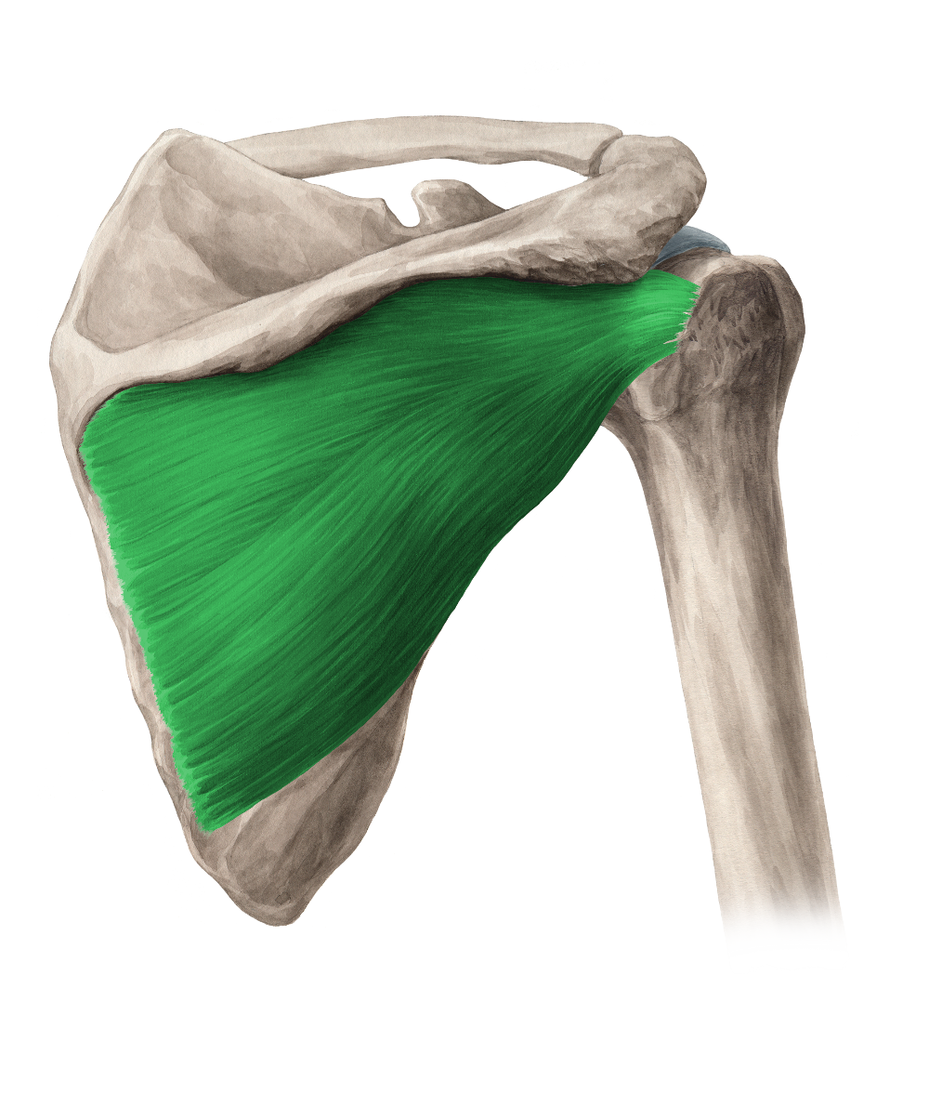
Until next time, Opus Fam! One of my favorite body parts to treat is the shoulder. Maybe because I relate to patients who have shoulder pain because of my own history, but maybe because it's like a puzzle with a ton of moving parts. The rockstar of the shoulder, of course, is the rotator cuff. But let's take a moment and talk about the often-times forgotten unsung hero - the Serratus Anterior. With 17 muscles attaching to the scapula (shoulder blade), it's really easy to get lost in the complexity of it. Everything has to work "just-so". When we look at how the shoulder moves as we raise our arms either out in front or to the side, our shoulder blades move as well. This scapular motion allows us to reach above our heads without pinching or putting more compression on the rotator cuff tendon. Source: Complete Anatomy So without further ado.... let's introduce the star of the show - the Serratus Anterior. 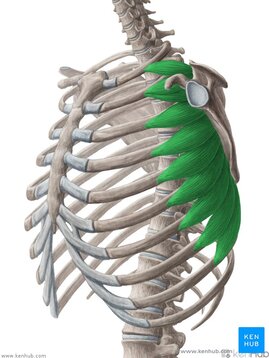 Source: Kenhub.com This amazing, broad muscle attaches on the underside of the shoulder blade (sandwiched between the ribs and the scapula) and inserts into the first 8 (of 12) ribs. It gets its name from the Latin root "serrare" - meaning "to saw" based on its jagged appearanace on the ribcage. When it contracts, it works to rotate the shoulder blade upwards and wrap around your torso as seen in the video above. If the shoulder blade didn't go through this rotation, it would actually contribute to pinching or impingement of the rotator cuff tendons in the subacromial space. The second function of the Serratus Anterior is that it keeps the shoulder blade close to the trunk. Without it, it would peel away, causing the shoulder blade to stick out or become more visibly prominent. Because your shoulder blade is not anchored by any ligaments except at the humerus and clavicle, it relies on the synchronization and stabilization through muscle co-contractions. People who have significant weakness in their serratus anterior will often exhibit more prominent, pronounced borders of their shoulder blades through movements of their shoulder girdle as seen in the video below. (hint: focus on the right side) While there are many exercises that are useful to help strengthen this all-important muscle, here is a quick and simple one that I like to give violinists/violists to help build the endurance of their shoulders to help them be able to hold their instruments up for longer periods of time. Remember - it is highly uncommon for a single muscle to work by itself without having other supporting players involved. The shoulder is no exception. 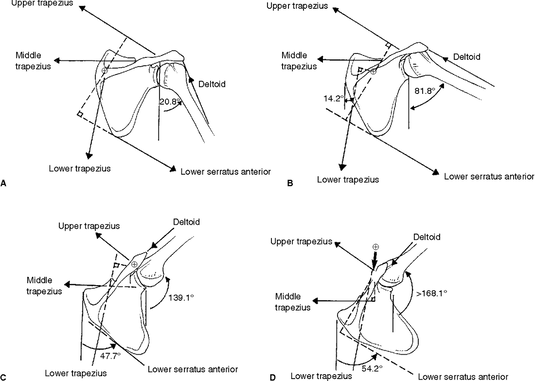 Source: Kibler BW, McMullen J. Scapular dyskenisis and its relation to shoulder pain. Journal of the American Academy of Orthopaedic Surgeons. 2003. Make sure that you take time to put in the effort to create good balance throughout your body, but particularly in the shoulder. Having a good, solid foundation at the shoulder blade will help you be able to move more freely and improve the overall dexterity in your wrist and fingers.
That's it for this week! Til next time.... Stay happy and healthy! Every time someone talks about 'core strengthening', your mind probably goes straight to "Abs! Abs! Abs!" and "Planks for days!" What if I told you that there is another often-neglected core in your body that is equally as important? Welcome to the fourth installment of our Posture Series. Allow me to introduce the Deep Neck Flexors (DNF) - Longus Colli and Longus Capitis. 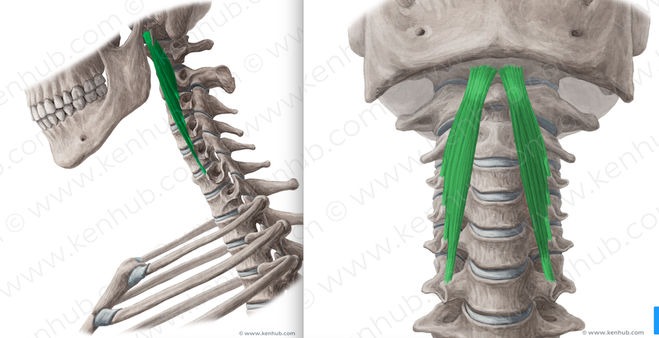 Image Credit: www.kenhub.com
Both of these muscles sit right up against your cervical spine and they work together to flex the spine to a small degree. When working together in a balanced manner in conjunction with the ALL of the muscles around your neck, including our friends the upper trapezius and suboccipitals which we discussed in previous posts, they help stabilize the head and neck through micro adjustments as you move. Neck pain and its effects on muscle activation of these muscles have been widely studied over the last few decades. Studies have found that up to 70% of patients with chronic neck pain actually have decreased muscle activation of the deep neck flexors and sternocleidomastoid (Source). In the same study, subjects with chronic neck pain who underwent a deep neck flexor strengthening program showed significant decreases in overall reported neck pain 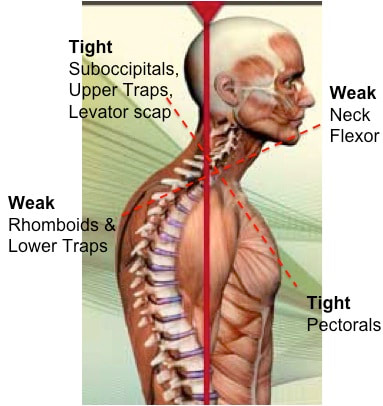 If you've read my last few blog entries, you are likely now familiar with our poor-postured friend. With poor posture, the DNF complex (the upper/front portion of the cross) gets stretched/elongated which, in turn, results in the muscles becoming inherently weaker and less able to perform the job it was tasked with. This is also significant for people who have experienced whiplash injuries such as being involved in a car crash. In the beginning of the whiplash motion, the head is flung backwards during the hyperextension phase (in the picture below), which strains the anterior neck muscles such as the DNF and sternocleidomastoid muscles (to be discussed in a future post). However on the rebound the head is flung forward, putting increased strain on the upper trapezius/levator scapulae muscles. Depending on the severity and velocity of impact, ligaments supporting the cervical spine may also become sprained. 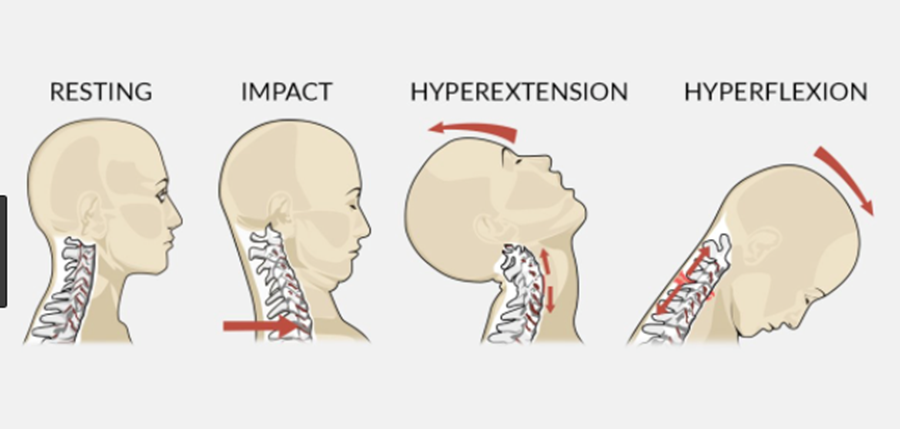 So you have a scenario of what came first? The chicken or the egg? Did neck pain develop which caused the DNF and supporting muscles to become weaker? Or did the DNF get weak because of poor posture, which resulted in neck pain?
This muscle is particularly important for musicians who are violinists or wind players. With the majority of mankind typically sitting in some kind of slouched posture you can end up relying on those stronger/tighter muscles that we previously discussed (upper trapezius much?) to support the instrument or bring our heads to the instrument to play. Instead, I challenge you to add in a bit of DNF strengthening into your warmup routine. Next week will be our final installment of the Posture series, where we spend a little more time with our poor postured friend and link some of these muscles together. While they are not the ONLY ones affected by posture, it's important to start to think about how they all affect each other and give you a better understanding of how they work. Until next time, Stay happy and healthy! [Muscle Monday] Nagging Shoulder Blade Pain Got You Down? - Consider the Rhomboid Major and Minor5/24/2020 Have you ever wondered why you may be getting pain between your shoulder blade and spine? For the second installment of our posture series, we will be discussing the Rhomboid Major and Minor. While they are two muscles, they almost always work together. Over the next few posts, we will be exploring some of the major muscles related to posture and how they work together. If you'd like to read our previous posts about posture, click here. Let's get things started. Allow me to present to you the Rhomboid Major and Minor: 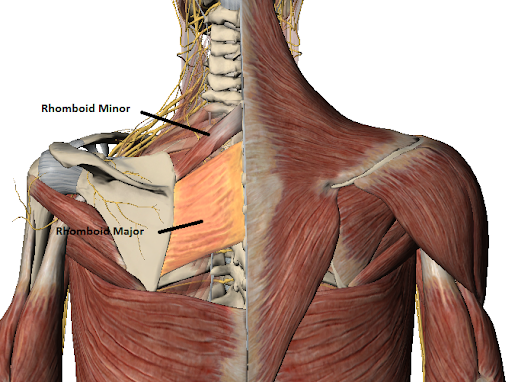 This dynamic duo attaches to from the spinous process of the last cervical segment (C7) and upper thoracic spine (T1-5) to the medial border of the shoulder blade. It sits one layer underneath the trapezius muscle, which we discussed in a previous post. The rhomboid minor is located superior/above the larger, broader rhomboid major muscle. Both work together to pull the shoulder blade towards the spine, otherwise known as "scapular retraction." Image source: Complete Anatomy This muscle is essential to the stability of the whole shoulder complex as it works to keep the shoulder blade supported during arm movements in all directions. The rhomboids can be a common source of pain in the area between the spine and your shoulder blade. Often times people will report pain, dull, aching or occasionally sharp pain to that region. This pain is very common in people who do a lot of prolonged work at a computer (particularly in the mousing hand), as well as musicians who have to hold their instruments in one position for long durations (flutists, violinists) One thing that should be acknowledged is that people can feel pain in other areas aside from the actual tissue source. The picture below demonstrates some common referral patterns where people may experience symptoms when there is a trigger point on the rhomboid ('X' marks the spot). 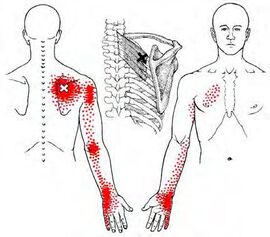 Image Source: Simons & Travell (1999) It is imperative that I warn you that 'trigger points' are not the only source of pain that can refer in this location or pattern. For example, there are joint-related pain that can also refer pain to similar areas. One of the most common ways that cues clinicians like me to suspect muscle-related/trigger point pain (other than palpating the muscle) is if patients often describe the pain as coming on after a prolonged period of time and they have to fidget around or change positions frequently to find a more comfortable posture. If you are unsure, be sure to seek out help from your friendly Physical Therapist (including us) to help you navigate this issue and help steer you back onto the right path. 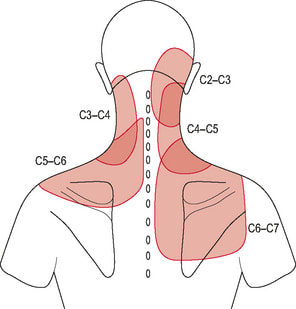 Cervical facet referral patterns We will discuss trigger points and what they actually are in an upcoming post. When looking at overall posture, these muscles are significant because when in a slouched posture, these muscles are commonly in a stretched position. This makes it more difficult for them to generate the amount of force needed to help hold the scapula in place. Remember this image? 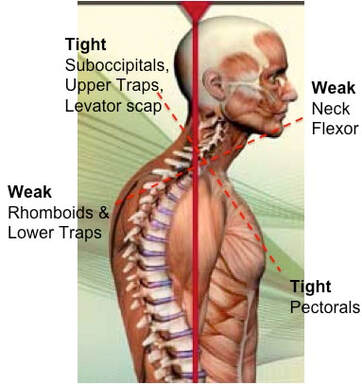 The harder these muscles have to work, the less time it takes for them to start to fatigue, which can be interpreted by your brain as that dull, aching sensation that you may feel.
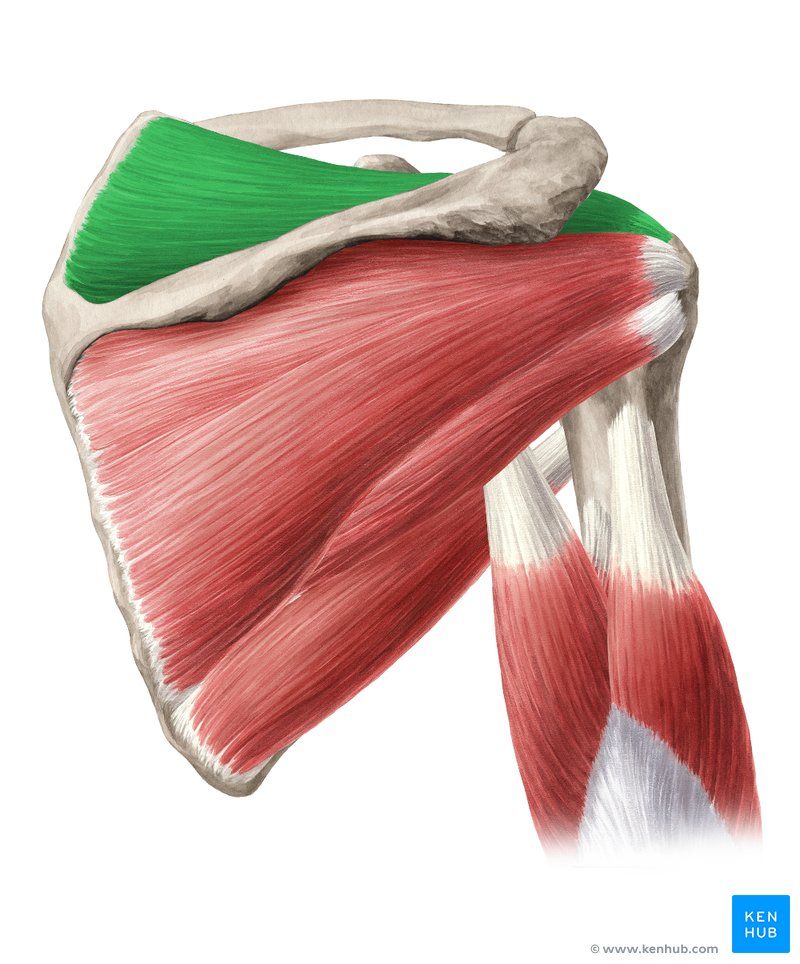
The best way to avoid this fatigue is to make sure that you have enough flexibility in the opposing muscles, such as the pectorals and the upper trapezius, and enough strength in the supporting muscles. Check out our post on Instagram for some ideas of some simple exercises you can do to get things moving in the right direction. Can't wait to share more about posture next week Until next time, stay happy and healthy! The next few episodes of Muscle Monday will be dedicated to discussing important muscles related to Posture. Questions about posture are probably one of the top things people ask me about on a regular basis, and the answer is not as simple as it seems. Posture involves many components which need to work together just-so in order to create the ideal scenario for your body to function at its best. Today, we will be talking about the might Pectoralis Major. 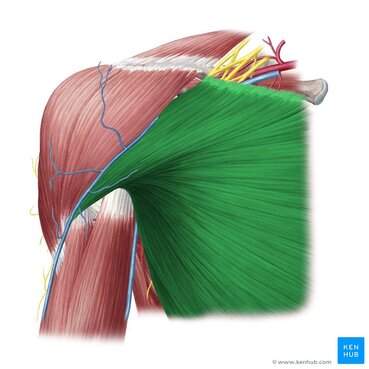 Photo Credit: Kenhub.com To say that this muscle is important would be redundant, because (almost) ALL muscles have a specific function, but this one in particular often gets a bad rep because it is associated with poor posture. In reality, it is an extremely versatile muscle that is used in most shoulder movements. Let's explore some fun facts about this muscle
Fact #2: The pec major can affect both the glenohumeral (shoulder) joint and the the scapula Due to its attachment on the clavicle, when the two portions of the pec major work together, they can depress the shoulder girdle Fact #3: The pec major performs movements in 5 planes of shoulder motion Because the muscle has two portions, the orientation of the muscle fibers allow it to move your shoulder in several planes of motion. The clavicular fibers assist with shoulder flexion while the sternal fibers assist with shoulder abduction AND extension. When the two portions work together, they will perform shoulder horizontal adduction, as well as shoulder (glenohumeral joint) internal rotation. Fact #4: Constantly sitting in a "slouched posture" will result in your pec major to get tight
Fact #5: In order to adequately take care of your body, you must do a combination of strengthening and stretching. It's all about balance. First of all, try and think about what positions you are in the most frequently and take the time to stretch in the opposite directions, no matter what that may be. Because most of us these days spend a lot of time sitting in front of a computer, on the couch or looking at our phones (or a combination of all 3?), you must make an effort to make sure that the muscle doesn't get too tight. Conversely, if you perform a task that requires a lot of pec use - such as playing a bowed instrument (Right arm), playing tennis, etc., you may want to invest a portion of your exercise routine to working on building strength, as it is also a key player in your overall shoulder stability. Take some time and check out this stretch to help improve your shoulder's powerhouse. Next week, we will be discussing the Pec Major's little brother, the Pec Minor. You're not going to want to miss it.
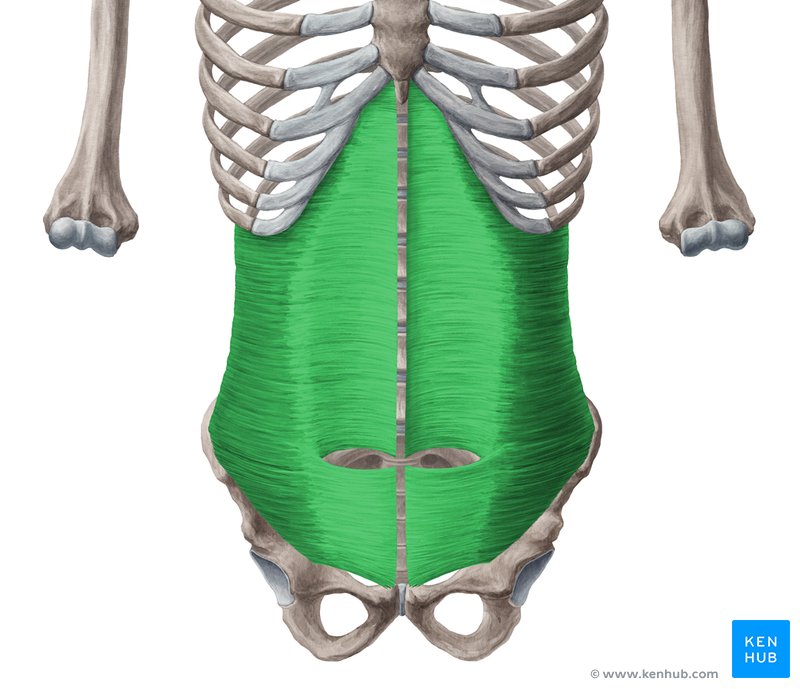
Until next time, stay happy and healthy! If you've been finding yourself sitting on the couch or at the computer for hours on end, this post is for you. So remember last post when I spoke about muscles seldom work in insolation? The same goes true for this week's featured muscle, but we'll just bring it back in and focus on our friend: The Transverse Abdominis I grew up playing tennis and practicing Tae Kwon Do. Later on in college, I rowed (much to my piano teacher's dismay --- my hands were ALWAYS blistered and torn up). What is the one thing during the workouts that ALL of my coaches (but none of my music professors) talked about? "You must strengthen the core"
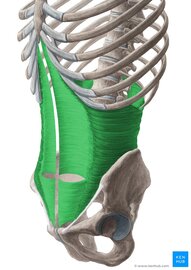
The Transverse Abdominis (TrA) is one component of the system of muscles that make up your core (stay tuned for further discussions regarding the core) The muscle is extremely broad - stretching across your torso. It attaches on the lower 6 ribs from the top, into the pubic bone on your pelvis. Medially, it attaches right down the middle of your abdomen via a facial junction and wraps around the sides and attaches into the fascia connecting to your abdominal obliques (internus).
Image Credit: Kenhub.com If you take a look at any of the other muscle pictures that I have posted, or even ones you can find online, understand that muscles will pull parallel to the orientations of its fibers. So in this particular case, they draw your stomach inwards like this:  It's not so much of a "sucking in your belly" type of motion, which is a common misconception. This is a 3D motion that occurs around your torso. Simplest way - if you've ever worn or seen a corset like they used to wear way back when, it's that kind of cinching together motion that this muscle performs.  Now, why is this significant? As the TrA contracts, it works in conjunction with other muscles in the back, pelvic floor in order to increase the pressure inside the abdominal cavity. That pressure will then push up against the lumbar spine to add even more stability. 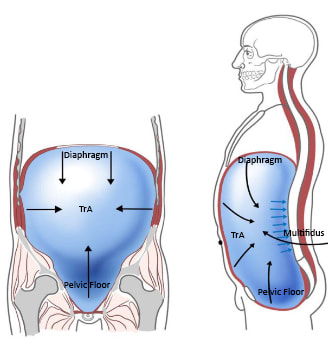 Whether you're walking, standing up from a chair, or raising your arm to retrieve an object, this core stability is essential in all aspects of human movement. In fact, it is so essential, that even as you reach out your arm to pick something up, your body anticipates the task and activates this system before it even happens. This means that your body should automatically engage all of the muscles before you even consciously realize that you're going to do it.
But wait.... There's more..... Many studies including this one and this O.G. study found that in subjects with low back pain, there was a delay in core muscle recruitment. We're not talking seconds or minutes, but even a millisecond delay can result in decreased core stability with performing a task (like a conductor starting his downbeat when no one is prepared) which ultimately can exacerbate the problem further, due to the lack of initial stabilization. This is a type of muscle that needs endurance training more-so than brute strength. So as you're going about your daily routine or workouts, see if you can feel your core kick on. Planks are a great place to start, but so are most fully body exercises because remember - you are never working out alone. Until next time, stay happy and healthy! So I'm going to cheat a bit and talk about 4 muscles instead of 1. Please forgive me (or not... your choice). Today, we are talking about a group of muscles that play an integral part of our shoulders and upper extremity strength. You might hear it as the "rotary cuff" or "rotator cup" (or a combination of the two) - the correct term is: Rotator Cuff. It consists of four muscles:
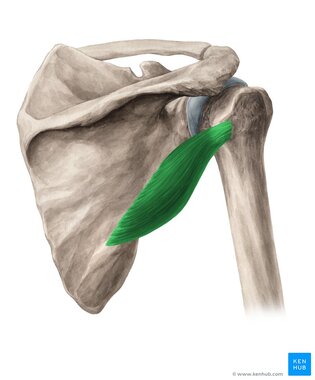
Image source: KenHub.com If we take a look at the shoulder joint in its simplest form - it is a ball and socket joint, much like your hip. The only difference is that the 'cup' portion - which is located on the scapula (the triangular bone) - is very shallow and does not provide much stability in and of itself. 3 muscles (supraspinatus, infraspinatus, teres minor) all work together to externally rotate the shoulder, while the subscapularis (on the front side of the scapula) works to internally rotate the shoulder blade. The four muscles also work together through the coordination of other muscles, not listed, to raise/abduct the arm to the side. One of the primary purposes of the rotator cuff is to work together so that when it contracts, it can pull the humerus into the socket to provide stability as your arm is moving.  You rely heavily on these muscles to help support your shoulder joint in its sweet spot through movement, but also if you are holding an object for a long period of time (violin, anyone?) Check out how the shoulder moves below, with the supraspinatus muscle highlighted: It is worth saying that it is relatively common for people to develop tendon-related issues over time, particularly with repetitive stress. As humans, we rely heavily on using our arms to perform daily tasks. It is one of the more common injuries in the shoulder and surgical rotator cuff repairs are one of the most commonly performed orthopedic procedures. BUT... Just because you may have problems that show up on a MRI, does not mean that you are guaranteed to have pain or problems, or must have surgery. Rotator cuff tears occur up to 40% of the population who are >60 years (Source). Within a population that had diagnosed rotator cuff tears, another study found that 65.4% of their sample group did not have ANY symptoms involving the shoulder. Take steps to strengthen the entire shoulder girdle as well as maintain your flexibility in order to prevent overuse and extra stress on your shoulder joint. Checking in with your local friendly physical therapist to help develop a prevention plan is a great place to start. If you don't have one, give us a call and let us know how we can help! If you want a few exercises to try out, give these a try! (remember, never perform or push through pain!)
That's it for this week. Until next time, stay happy and healthy!
When I was in college, there was a wellness fair with a massage station tucked away in the corner of the cafeteria. I waited patiently for my turn and when it came, the therapist introduced herself to me and asked me if there were any areas I wanted her to work on. I had never received a professional massage before, so I just shrugged and told her to focus on wherever she thought was the best. She smiled and had me sit and put my face in the hole in the massage chair. When she felt my shoulders, she recoiled in horror and called her colleague over to feel my muscles as well. "WHAT are you doing to yourself??!" they asked. The fact is, is that I was on the computer, playing the violin and piano and texting for hours upon hours during the day. I had build up so much tension, but I didn't even realize it. Allow me to introduce you to our friend, the Upper Trapezius: 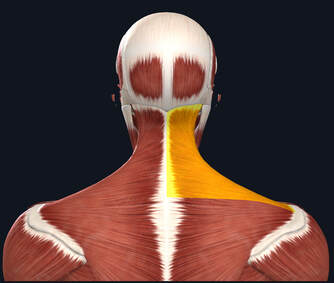 This broad muscle attaches from the base of your skull, extending down the spine and out through the upper border of your shoulder blade. It's part of It's responsible for controlling your head and neck. What's more important, is that it's a common muscle to exhibit tightness as a result in poor posture, stress or anxiety. The upper traps can also contribute to neck pain, headaches or pain in the shoulder blade. These tender areas are commonly referred to as "trigger points", which we will discuss in a future post. 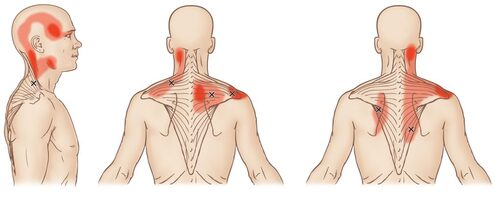 Simons, D. G., Simons, L. S., & Travell, J. G. (1999). Travell & Simons' myofascial pain and dysfunction: The trigger point manual. Baltimore: Williams & Wilkins. Here are 3 things that you can do to help improve the tightness of these muscles.
If you have any pain that persists or not sure how to stretch, make sure you seek help from a physical therapist or medical professional for the best guidance.
Until next time, stay happy and healthy! |
AuthorDr. Janice Ying is a Los Angeles-based Physical Therapist. She is board-certified Orthopedic Physical Therapy Specialist and is regarded as a leading expert in the field of Performing Arts Medicine and the development of cutting edge injury prevention and rehabilitation programs for musicians. DisclaimerThe information on this website is intended for educational purposes and should NOT be construed as medical advice. If you have or think you have a health-related issue which needs to be addressed, please seek the help from your local licensed medical professional.
Archives
October 2020
Categories
All
|
||||||||||||||
MOBILE AND TELEHEALTH
PHYSICAL THERAPY
AND WELLNESS SERVICES



 RSS Feed
RSS Feed
We would love to see you soon!
|
© Opus Physical Therapy and Performance - 2021 - All Rights Reserved